How does the epithelium contribute to asthma pathology and symptoms?
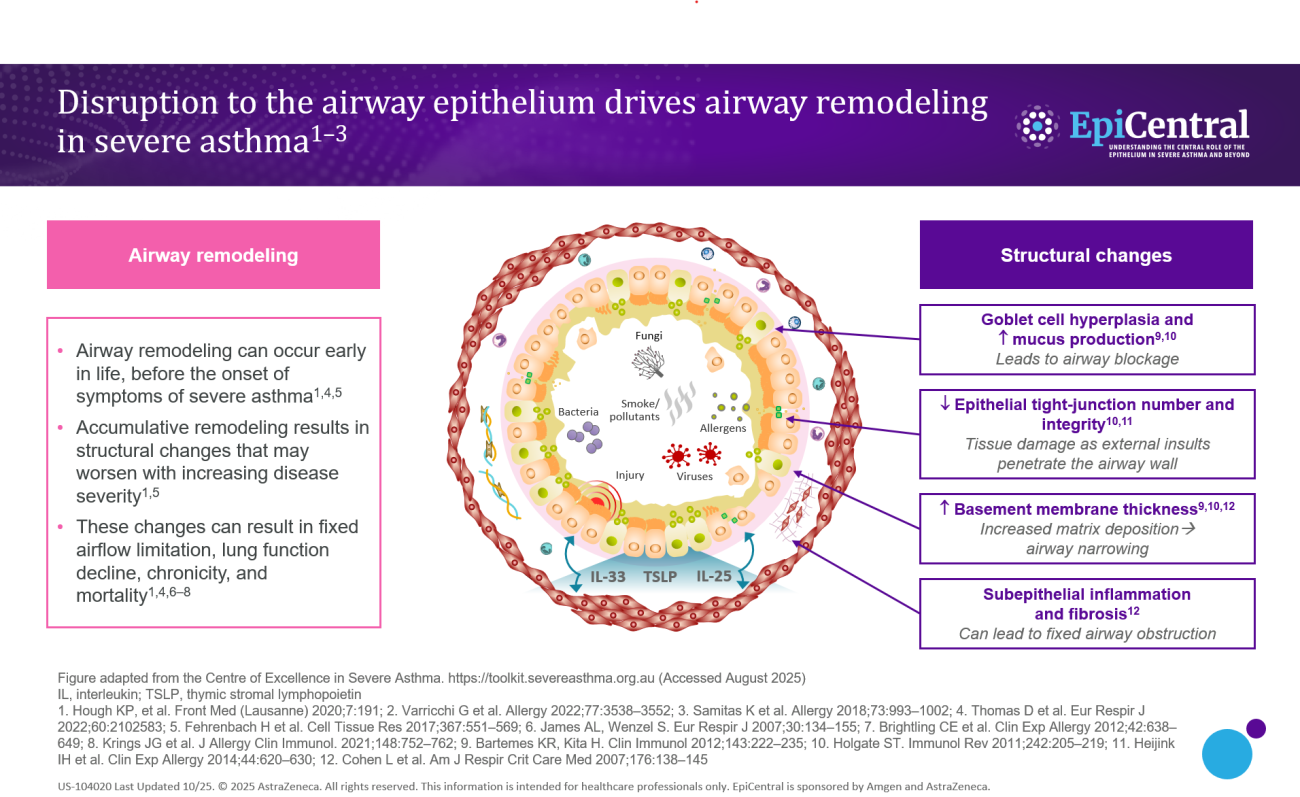
In addition to marked airway inflammation, structural changes to the airway epithelium are also observed in asthma (Figure 1), rendering the airways more vulnerable to infection and environmental triggers.4 Both the extent of inflammation and structural changes influence the severity of the disease and asthma symptomatology.3
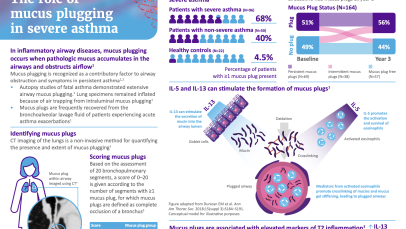
Structural changes include goblet cell hyperplasia,3,4 and, in more severe disease, a change in mucin expression, primarily an increase in the Mucin 5AC (MUC5AC) to Mucin 5B (MUC5B) ratio, resulting in an MUC5AC-rich mucus that tethers to epithelial mucus cells and markedly impairs mucociliary transport.15 This increase in submucosal goblet cells and mucus plugging can lead to airway blockage.3,15
There is also a decrease in the number and integrity of tight junctions,2,3 that may cause tissue damage as external triggers are able to penetrate the airway wall.
Increased epithelial thickness4,7 and subepithelial fibrosis7 have also been observed, resulting in airway narrowing and fixed airway obstruction, respectively.
Finally, there are increased levels of inflammatory cells (including mast cells and eosinophils),16,17 which, in turn, can cause heightened inflammation and airway hyperresponsiveness.